_edited.jpg)
5 Common Causes (+ Solutions) to Hair Loss & Thinning
- Drew Dreiling
- Jun 11
- 9 min read

HAIR LOSS & THINNING IS THE NORM- BUT IT DOESN’T HAVE TO BE
A healthy scalp and full head of hair contains approximately 100,000 hairs and hair follicles, and even a healthy scalp sheds 50-100 hairs a day as part of the natural hair growth cycle.

However, over >80% of U.S. men and >30% of U.S. women will experience significant hair loss (alopecia) and hair thinning in their lifetime. [1]
And while many people write off hair loss as “genetic” and inevitable, emerging research shows that modifiable lifestyle factors and medical treatments often play the most significant role in hair loss and hair health.
For instance, Androgenetic Alopecia, the most common type of hair loss, is driven in large part by DHT (dihydrotestosterone) levels, a modifiable biomarker.
Alopecia Areata and Cicatricial Alopecia are two forms of hair loss driven by inflammation and autoimmune conditions (including Hashimoto’s thyroiditis and lupus), of which there are several effective therapeutic interventions for.
Telogen Effluvium, a form of hair loss that’s on the rise in the U.S., is driven by periods of stress, certain illnesses (ex. COVID), and childbirth.
Another form of Effluvium- Anagen Effluvium, causes an interruption in the growth phase of the hair follicle (anagen phase) and is often caused by chemotherapy or radiation.
Traction Alopecia is hair loss caused by physical tension on the hair (ex. wearing tight ponytails, braids or weaves).
And Tinea Capitis is hair loss caused by a fungal infection of the scalp, which is most common in children.
So while genetic factors often play a role, modifiable lifestyle factors and medical treatments can often slow or even completely reverse hair loss and thinning in many cases.
5 COMMON CAUSES (+ SOLUTIONS) TO HAIR LOSS & THINNING
Below are 5 common causes, along with some possible solutions, to hair loss and thinning (I’m not discussing hair transplantation here).
With hair improvement approaches like this, it's very important to keep in mind that it's a process.
Generally the first 2-3 months a person won't see a lot of visible results, and they may in fact see more shedding. Some even call this the Shedding Phase. This is because the weak hair follicles often release older and weak hair to make way for newer, stronger hair coming from a rejuvenated hair follicle.
Months 3-6 are where most should see some new growth and improved hair strength and thickness (Growth/Improvement Phase). And the best results are generally seen after 6 months (Visible Results Phase).
The specific hair health strategies below are in addition to a healthy lifestyle, which includes…
a healthy diet
regular exercise
stress reduction & healthy coping mechanisms
no smoking (85% of smokers experience hair loss vs 40% of non smokers) [1]
and healthy sleep habits
… all contributing to improved metabolic health and lower chronic inflammation.

POTENTIAL CAUSE #1:
HIGH BLOOD SUGAR & INSULIN
Emerging research links high carbohydrate and sugar intake (especially sugary drinks) with a 57% greater risk of early pattern hair loss. [2]
Tests for blood sugar and insulin include:
A1c (target 4.7-5.3%)
insulin (target <8 mIU/L)
CGM/continuous glucose monitor (target 70-90 mg/dL fasted, <140 the 1-2 hrs after eating)
General therapies here include:
lower carbohydrate intake (<100g/day)
higher protein intake (>100g/day)
regular strength training (2-6x/wk)
berberine supplement (500mg 1-3x/day)
GLP-1 medications (semaglutide, tirzepatide, retatrutide)
GLP-1 related meds are generally taken via injection once a week.
The starting dose of semaglutide (agonist of GLP-1 hormone) is 0.25mg and after 4 weekly injections can be titrated up. Higher doses include 0.5mg, 1.0mg, 1.7mg, 2.0mg (max for Ozempic/T2D med), 2.4mg (max for Wegovy/obesity med). Many will titrate up to either 1.0mg or 1.7mg.
The starting dose of tirzepatide (agonist of GLP-1 & GIP hormones) is 2.5mg and after 4 weekly injections can be titrated up. Higher doses include 5mg, 7.5mg, 10mg, 12.5mg and 15mg (max dose for both Mounjaro/T2D med and Zepbound/obesity med). Many will titrate up to 10mg and stay at that dose.
The starting dose of retatrutide (agonist of GLP-1, GIP & glucagon hormones) is not standardized as the drug is still in phase 3 trials (as of summer 2025) but a common starting dose is 1mg and after 4 weekly injections can be titrated up. Higher doses include 2mg, 4mg, 6mg, 8mg. Up to 12mg/wk have been used in clinical trials. Therapeutic dose for most will be 2-8mg/wk.

POTENTIAL CAUSE #2: OTHER HORMONE IMBALANCES (INCLUDING HIGH DHT & LOW THYROID HORMONES)
Tests here include:
Total testosterone (target 700-1100 ng/dL for men not on TRT & 40-90 for women not on TRT)
DHT (target 30-50 ng/dL for men and 5-20 for women)
TSH (target 0.5-2 mIU/L unless taking iodine, which will temporarily spike TSH)
free T4 (target 1.3-1.8 ng/dL)
free T3 (target 3-4.5 pg/mL)
For many women, PCOS (polycystic ovarian syndrome) causes higher than normal testosterone levels, which often leads to high DHT levels resulting in scalp hair loss & thinning (and unwanted hair growth on other parts of the body). A transvaginal ultrasound can confirm if PCOS is present.
Therapies for reducing and modulating DHT levels include oral saw palmetto, topical dutasteride + minoxidil, and topical spironolactone + minoxidil.
For oral saw palmetto, dosages are generally 320-640mg/day of a saw palmetto standardized to 85-95% fatty acids (max dosages are 960mg/day).
Topical dutasteride is appropriate for all adult men as well as women over 50 years old. Concentration of topical dutasteride is 0.1-0.3% and generally 1.0 mL is applied topically to the scalp 2x/day (AM & PM). I don’t recommend oral dutasteride due to the increased likelihood of side effects. [3]
Topical spironolactone is appropriate for women under 50 years old. Concentration of topical spironolactone is often 0.5% and generally 1.0 mL is applied topically to the scalp 2x/day (AM & PM). I don’t recommend oral spironolactone due to the increased likelihood of side effects. [4]
Therapies for improving circulating thyroid hormone levels in hypothyroid patients include:
iodine (1-12.5mg/day) + tyrosine (1,000-3,000mg/day)
NDT (natural desiccated thyroid containing T4 + T3 such as Armour, generally 30-120mg in AM)
synthetic T4 (levothyroxine, generally 25-75mcg but may go as high as 150mcg)
synthetic T3 (liothyronine, generally 5-25mcg, often combined with levothyroxine)

POTENTIAL CAUSE #3:
INFECTION, INFLAMMATION
Infection can often lead to chronic inflammation, and conversely inflammation can exacerbate certain illnesses.
Tests for common gut, lung and systemic infections include:
GI Map (for infections in the gut) [5]
blood culture
STD/STI tests
COVID tests [6]
All of these can be ordered online.
A respiratory culture (sputum) test can also be ordered by a provider.
For scalp infections like Malassezia, candida and ringworm/tinea, a KOH prep test may be run, often by a dermatologist, to identify if a fungal infection is present and what type of fungal infection it is (test results are often available in minutes). [7-8]
Tests for inflammation include CRP (target <3 mg/L) and homocysteine (target 4-8 µmol/L).
Therapies for addressing mild to moderate gut & systemic infections, which may be parasitic, bacterial, fungal or viral may include functional meds such as ivermectin, fluconazole, valacyclovir or supplements such as oregano oil, goldenseal root, monolaurin, undecylenic acid, elderberry. Note that long term use (>2 months) of high dose fluconazole (>400mg/day) may actually cause alopecia in some people. [9]
Additional immune support is often needed for infections, which include probiotics, vitamins C, A, D3 plus zinc.
Therapies for scalp infection often include ketoconazole shampoo (often 2-3x/week) and sometimes ketoconazole cream (often applied daily). For shampoo, 1% ketoconazole is available OTC while 2% is available with a prescription (ex. through RedBoxRx online). I don’t recommend oral ketoconazole due to increased likelihood of side effects. [10-11]
A pure aloe vera product can be applied to the scalp after shampooing to help soothe irritated skin.
Therapies for inflammation often include:
higher dose curcumin (turmeric standardized to 95% curcuminoids, often 2,000-4,000mg/day)
higher dose omega 3 (2,000-4,000mg of DHA+EPA per day)
periodic fasting (>24 hours without caloric intake one or more times a month)
POTENTIAL CAUSE #4:
NUTRIENT DEFICIENCIES
Several nutrients are needed for healthy hair follicles and hair health. [12-14]
Most of these nutrients play an essential role in either collagen and/or keratin production. Nutrients here include:
protein (including collagen protein)
biotin (needed for keratin)
iron (needed for keratin and RBC & oxygen transport)
silica (essential for collagen production)
zinc (regulates DHT, supports keratin, essential for DNA, RNA, protein synthesis)
Dietary protein insufficiency can sometimes be determined from biomarkers like total protein, albumin and creatinine (although the first two can be low in cases of liver disease as well).
Biotin as a biomarker is rarely run, as it is prohibitively expensive.
Iron status can sometimes be determined from ferritin (target 70-200 ng/mL), however, ferritin is an acute phase reactant and can be elevated if significant infection, illness or inflammation is present. Therefore, it’s best practice to also look at CRP (inflammation marker) along with other iron markers (TIBC, transferrin saturation % and serum iron).
A silicon test (silicon is the elemental form of the compound silica) can be run to determine blood levels but, like biotin, is rarely run due to cost.
A zinc test can be run to determine zinc levels but it is rarely run, despite a reasonable out of pocket cost (around $50).
Therapeutic interventions with these nutrients often look like the following:
protein: >100g/day (and >20g collagen peptides supplement)
biotin: 5,000-10,000 mcg (5-10 mg)
iron: for a bioavailable form such as ferrous bisglycinate, aim for 25-65mg twice daily (50-130mg/day)
silica: for the most bioavailable forms (orthosilicic acid or mono-methyl-silane-triol/MMST) aim for 10-20mg of silica/day, for less bioavailable forms such as silica found in horsetail supplements, aim for 35-80mg of silica/day
zinc: 30-60mg/day (look for supplements that also contain 2mg of copper for every 15-30mg of zinc)
Other nutrients playing a supportive role in hair health include vitamins C (needed for iron absorption), A and D.
Note that copper supplementation can help reverse grey hair in some cases.
POTENTIAL CAUSE #5:
POOR SCALP CIRCULATION & HEALING FACTORS
Poor scalp circulation and low levels of healing factors (ex. stem cells, growth factors, etc.) can negatively impact hair follicles and hair health. Therapies that can improve scalp and hair follicle health via improved circulation and/or increased availability of healing factors include…
Scalp massage: manual stimulation to improve localized blood flow
Titanium microneedling derma roller: creates controlled micro injury to the skin which solicits a healing response, often using a roller with 0.25mm size needles 2-3x a week (derma rollers available on Amazon for <$10, and should be replaced after 10-15 uses) [15-16]
Topical minoxidil: a vasodilator that improves blood flow to hair follicles, over-the-counter concentrations are usually 5% with stronger concentrations, like this 8% minoxidil product from Happy Head that also includes dutasteride, available via prescription; usually 1 mL applied 1-2x/day [17]
Red & Near Infrared Red (NIR) light therapy: red and NIR light therapy using a laser or LED (sometimes called PBM or LLLT) has been shown to reduce chronic inflammation and improve mitochondrial functioning and circulation, leading to healthier hair follicles and healthier hair [18-19]
Platelet rich plasma (PRP): platelets found in plasma, especially super concentrated platelet rich plasma (SC-PRP), contain growth factors that can help rejuvenate hair follicles (often used for chronic joint pain conditions) [20-21]
Exosomes: cell-free nanoparticles (~30–150 nm) secreted by stem cells, exosomes have been successfully used for hair restoration as well as chronic joint pain conditions [22]

PUTTING IT ALL TOGETHER
Identifying the cause (or causes) of hair loss is step #1. After that, selecting the best therapeutic interventions and then consistently executing them over at least 6 months is what generally brings the best results.
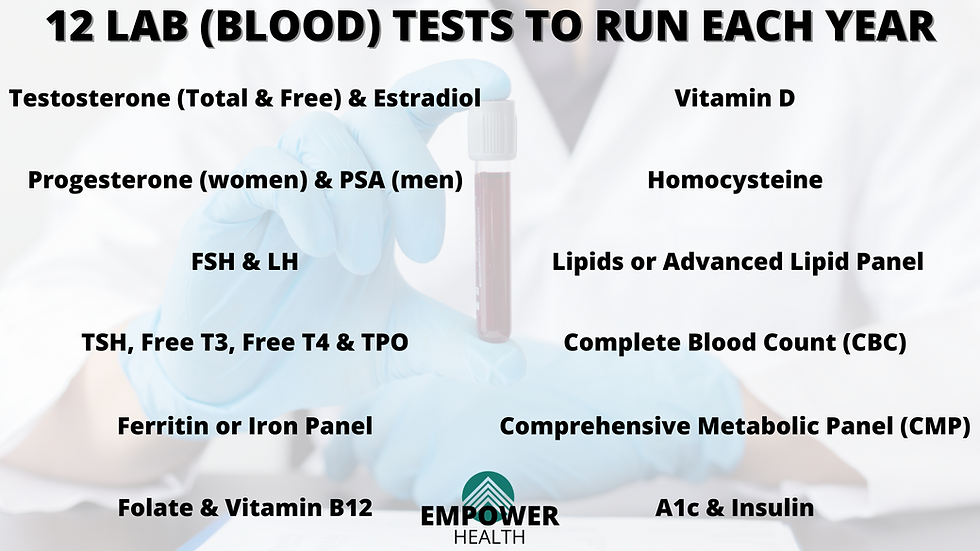
At a minimum I suggest testing for A1c (3 month blood sugar), thyroid hormones (free T4 and free T3), DHT and ferritin (often the most useful marker for iron status).
Here is a summary of some of my preferred hair health interventions:
High protein, low carbohydrate diet
Berberine if A1c is mildly elevated or GLP-1 med if A1c moderately or severely elevated
Oral saw palmetto (especially if DHT is elevated)
Lower dose of iodine (1-3mg/day) unless hyperthyroid/Grave’s
1% ketoconazole shampoo 2-3x/wk, especially if scalp dandruff or seborrheic dermatitis present (can apply aloe vera after shampooing)
High dose curcumin if inflammation present
Default hair health supplement stack: biotin, silica, zinc with copper
Gentle iron (+ vitamin C) if iron deficiency present
Microneedling derma roller 2-3x/wk plus daily application of topical hair growth serum (ex. minoxidil + dutasteride for all men and women >50 or minoxidil + spironolactone for women <50)
Note that of all the interventions discussed, exosomes are by far the most expensive treatment option (often $3,000 or more per treatment session) followed by PRP (often $500 or more per treatment session).
A common treatment protocol for both exosomes and PRP is 1 treatment a month for 3-6 months.
What I recommend for most of my clients is they stack the more affordable interventions and execute those for at least 3-6 months before considering either PRP or exosome treatment.
SOURCES

Comments